
The Brain’s Reward Pathway: What Changes in Depression and ADHD?
People often talk about the brain’s reward pathway as if it were a single pleasure button. That is simple, memorable, and mostly wrong.
The human brain does not run on pleasure alone. What we call the reward pathway is really a set of brain circuits that help us notice what matters, predict what might feel worthwhile, and decide whether something is worth the effort. It is involved in motivation, learning, and action, not just enjoyment. The strongest models place the ventral tegmental area, often called the (VTA), and the ventral striatum, which includes the nucleus accumbens (VS-NAc), near the centre of this network. These regions are especially important for reward learning, motivation, value, and effort-based decision-making.
That matters because when people say, “This is just a dopamine problem,” they usually mean something too simple. Dopamine is important, but it is not the same thing as pleasure. A useful way to think about dopamine is that it helps the brain learn what is worth pursuing, energise behaviour, and update expectations. In other words, it is deeply involved in wanting, effort, and learning, not only in liking.
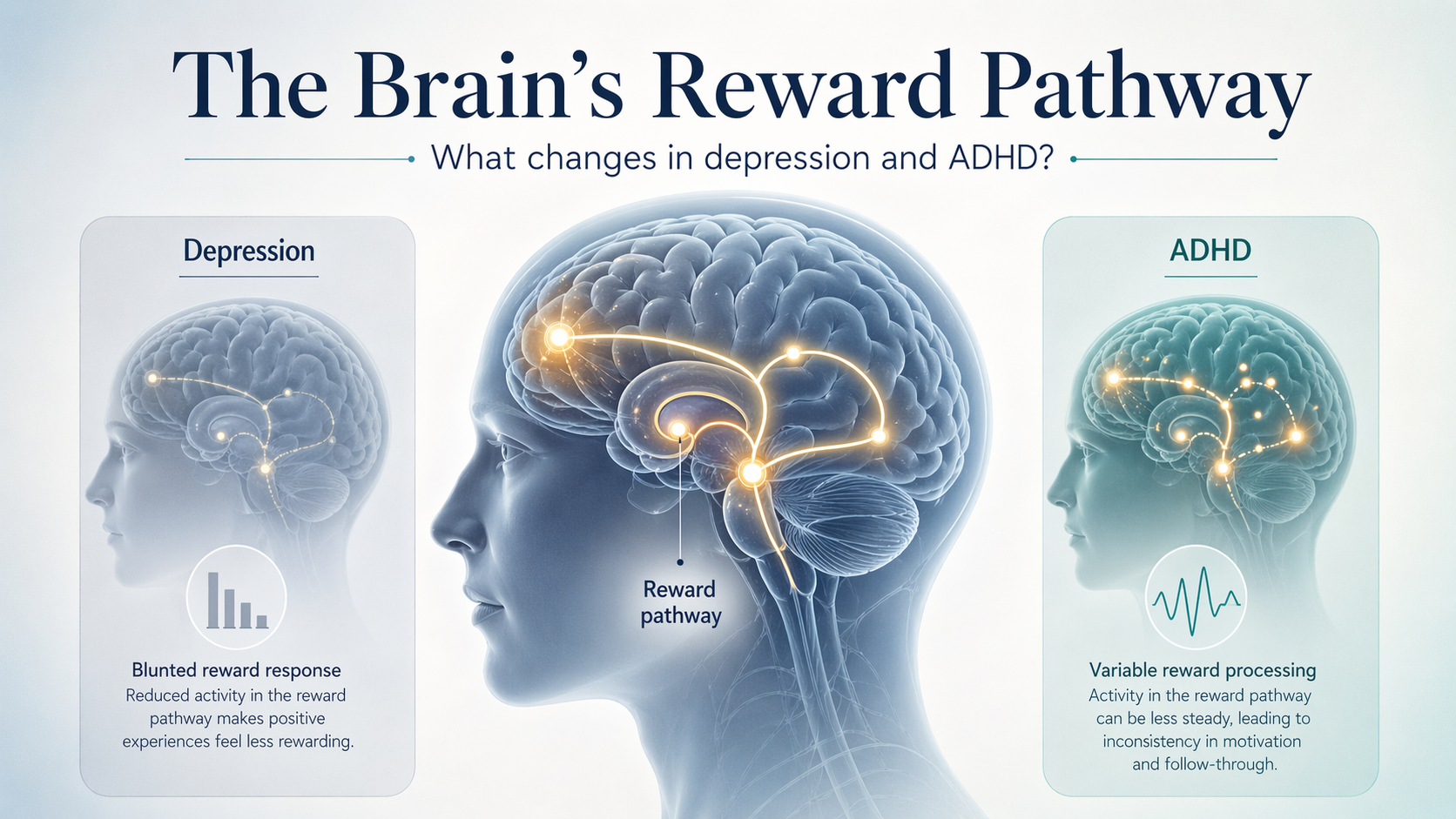
This is where depression and ADHD become interesting. Both can affect reward processing, but they do not do so in the same way. In depression, the reward system often looks less responsive. In ADHD, it often looks less steady, less well tuned to timing, and more drawn to what is immediate.
What the reward pathway is, in plain English
The reward pathway is not one wire running from pleasure to happiness. It is a network. Different parts of the network do different jobs.
The VTA, deep in the midbrain, sends dopamine signals to other regions. The (VS-NAc) helps turn those signals into motivated behaviour. Prefrontal areas in the brain help weigh options, judge value, and decide whether the likely reward is worth the effort. Together, these circuits help answer a set of practical questions: Is this important? Is it worth doing? How hard should I work for it? What should I learn from the outcome?
This is why “reward” in neuroscience is broader than pleasure. It includes anticipation, effort, value, reinforcement learning, and action selection. You may enjoy a reward when it arrives, but the system also has to help you notice the cue, prepare for the reward, choose the action, and learn from what happens next.
That is also why dopamine should not be treated as a simple happiness chemical. The older and stronger literature suggests that dopamine is especially important for motivation and incentive salience, meaning the brain’s sense that something is worth chasing. Pleasure itself involves a wider set of systems. So when dopamine changes, the problem may show up less as “I cannot feel anything at all” and more as “I cannot get going,” “I cannot stay interested,” or “My brain is not treating this as worth the effort.”
What changes in depression
In depression, the most consistent evidence is not simply low happiness. It is altered reward processing, often in a blunted direction.
A large behavioural meta-analysis in JAMA Psychiatry found that depression was associated with overall impairment in reward processing, with especially clear problems in reward bias, option valuation, and reinforcement learning. In simple terms, this means the depressed brain may be less likely to favour rewarding information, less able to judge that an option is worth pursuing, and less efficient at learning from reward.
This fits well with the clinical idea of anhedonia, but anhedonia is often misunderstood. It is not only about enjoying things less once they happen. It can also mean that rewards feel less motivating in advance, less able to pull behaviour forward, and less worth the effort. A person may say, “I know this used to matter to me, but now my brain does not seem to move toward it.”
Brain imaging adds an important layer. A neuroimaging meta-analysis found that major depressive disorder was associated with reduced responses to reward in the ventral striatum, while some regions (orbitofrontal) showed the opposite pattern. That does not mean depression is a single lesion in one spot. It means the network handling reward and value appears dysregulated, with the ventral striatum showing a reliable reduction in reward-related response.
If we stay focused on the VTA-ventral striatal part of the network, the picture becomes clinically useful. These circuits are involved in motivation, expected value, learning from reward, and deciding whether effort is worthwhile. In depression, they often seem less responsive to reward signals. That helps explain why everyday goals can start to feel flat, distant, or strangely effortful.
What changes in ADHD
ADHD is different. It is tempting to reduce it to “low dopamine,” but that is too neat to be reliable.
A major 2024 review concluded that dopamine is clearly involved in ADHD, but the evidence does not support a simple global hypo-dopamine model as the main explanation. That is an important correction, because the real picture appears more uneven and context-dependent.
Even so, there are some repeated findings. A meta-analytic review of fMRI studies found ventral striatal hyporesponsiveness during reward anticipation in ADHD. In plain English, many ADHD groups show a weaker ventral striatal response when the brain is preparing for a possible reward. That matters because anticipation is a major part of motivation. If the cue for a future reward does not register strongly enough, it is harder for the brain to mobilise effort early.
ADHD also seems to involve altered reinforcement learning in at least some studies. A 2024 study found reduced sensitivity to reinforcement and blunted ventral striatum signals during flexible reward learning in ADHD. This does not mean every person with ADHD has the same pattern, but it does support the broader idea that reward learning can be altered.
Another repeated theme is timing. Reviews continue to show that ADHD is often linked to steeper delay discounting, meaning a stronger pull toward smaller immediate rewards over larger delayed ones. This does not mean people with ADHD do not care about long-term goals. It means the brain may give less weight to rewards that are distant in time, especially when they are abstract, delayed, or poorly signalled.
So the contrast with depression is important. In depression, the reward system often looks blunted, especially around valuation and reinforcement learning, and the whole process can feel flat and effortful. In ADHD, the system often looks less stable in timing and anticipation, with many studies pointing to weaker ventral striatum responses to future reward and a stronger attraction to what is immediate. Both conditions can reduce motivation, but they may do so for different reasons.
Why this matters
The public conversation often turns these conditions into slogans. Depression becomes “low dopamine.” ADHD becomes “a dopamine deficiency.” Social media loves short answers, but the science is more careful than that.
The reward pathway is a network, not a pleasure button. Dopamine matters, but it is not the same thing as pleasure. The VTA and ventral striatum are central because they help the brain learn what matters, estimate value, prepare effort, and move toward reward. When these circuits change, the result is not a moral failure. It is a shift in how the brain handles motivation, value, and action.
That is why the language we use matters. A person with depression is not simply failing to cheer up. A person with ADHD is not simply failing to try harder. In both conditions, parts of the reward system may be working differently. The details are not identical, but the core point is the same: these are brain-based difficulties in motivation and reward processing, not defects of character.
Note: Some concepts in this article are simplified to make the science easier to understand without changing the main message.